Atrocities of two German neuropathologists Julius
Hallervorden and Hugo Spatz during Second World War are notorious. The
eponymous term Hallervorden –Spatz syndrome is disfavoured and
neurodegeneration with brain iron accumulation (NBIA) is encouraged.
Ante mortem diagnosis of this rare condition is made
possible with the use of MRI examination. Two distinct clinical presentations
are described one is classical form and another is atypical variant based on
the age of onset. Both the forms are progressive with poor prognosis.
Patients present in early age with progressive gait
impairment, rigidity of all limbs, dysarthria and mental retardation.
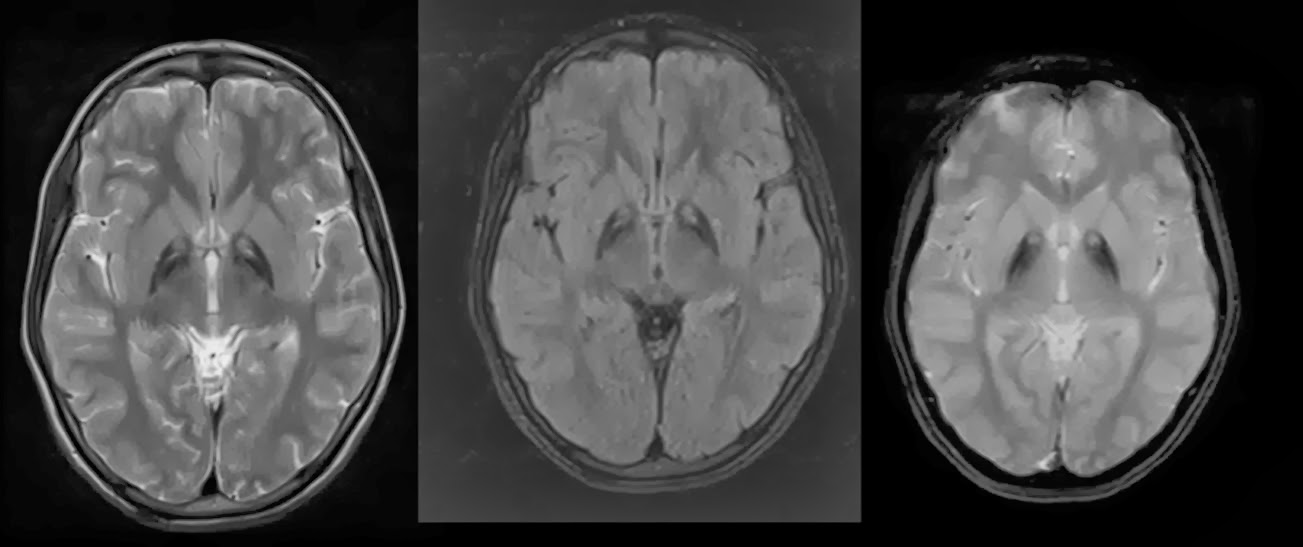
MRI findings are striking and reflect the pathology.
Preferential deposition of the iron in globus pallidus will result in its
destruction. The MRI appearance is described as eye of the tiger appearance.
This sign is seen in both T2W and FLAIR imaging. Foci of T2 Hyper intensity
noted with in the area of T2 Hypo intensity. Hypo intensity reflecting the iron
deposition and the hyper intensity reflecting the gliosis changes.
Ref:
.bmp)

